by Gemini Pro AI. Lightly edited by Nathan Beel 2026
The inclusion of diploma-qualified practitioners (AQF Level 5) in the Australian counselling profession is a central and often contentious point of debate. This tension is primarily embodied by the two peak bodies: the Australian Counselling Association (ACA), which provides a professional home for diploma holders, and the Psychotherapy and Counselling Federation of Australia (PACFA), which maintains a minimum entry standard of a Bachelor’s degree (AQF Level 7).
As Australia faces a growing mental health crisis, the role of the VET-trained (Vocational Education and Training) counsellor is being reassessed through the lens of workforce capacity, clinical safety, and professional identity.
1. The Pros (Advantages)
A. Substantial Increase in Workforce Capacity
The most immediate benefit is the volume of practitioners available to enter the sector. Australia’s mental health system is currently under extreme pressure, with wait times for psychologists and psychiatrists often exceeding six months in metropolitan areas.
Speed to Market and Agility: A Diploma of Counselling (CHC51015) can be completed in 12–18 months. This rapid turnaround allows the workforce to scale in response to national emergencies. For example, during the COVID-19 pandemic and the Black Summer bushfires, the surge in psychological distress required an “all-hands-on-deck” approach. Diploma graduates provide a scalable “middle tier” that can be deployed faster than university graduates.
Addressing the “Missing Middle”: Many Australians do not require intensive clinical interventions for every issue. Diploma holders fill critical gaps in “frontline” services—NDIS support coordination, youth mentoring, crisis hotlines, and community-based intake roles. By handling these foundational support needs, they prevent the higher-tier clinical workforce from being overwhelmed by non-clinical caseloads.
B. Socioeconomic Diversity and Cultural Representation
The university system, while prestigious, remains a significant barrier to entry for many who possess the natural temperament and life experience required for effective counselling.
Democratizing the Profession: Lower tuition costs and the availability of VET Student Loans make the career path accessible to people from lower-income backgrounds. This prevents the profession from becoming an “elite” bubble.
The Power of Lived Experience: Many diploma students enter the field as a second career, often motivated by their own “lived experience” with recovery or trauma. This background fosters a level of empathy and “on-the-ground” relatability that is highly effective in peer-support models.
2. The Cons (Disadvantages)
A. Professional Credibility and the “Perception Gap”
The primary argument against diploma inclusion is that it inhibits the professionalization of counselling, keeping it in the shadow of more strictly regulated fields like psychology.
The Medicare Obstacle: The Federal Government has historically used the lack of a “minimum degree standard” as a reason to exclude counsellors from the Medicare Benefits Schedule (MBS).
Inter-Professional Skepticism: GPs and psychiatrists may be hesitant to refer patients to a “Counsellor” if they cannot be certain of the practitioner’s training level, leading to a general lack of trust in the title itself.
B. Gaps in Theoretical Depth and Clinical Nuance
A significant risk of shorter, vocational training is the “unknown unknowns”—practitioners who may lack the theoretical framework to recognize when a client’s needs exceed their competency.
Limited Research Literacy: Diploma graduates typically do not receive training in evidence-based practice evaluation or the ability to critically appraise new clinical research.
Risk of Misdiagnosis: Without deep training in developmental psychology and psychopathology, a practitioner might miss the subtle signs of complex personality disorders or severe dissociation.
3. Solutions: Reducing the “Cons” and Mitigating Risk
To maintain the benefits of a diverse, agile workforce while addressing the risks of lower-tier qualifications, several strategic solutions are being implemented or proposed within the Australian sector.
A. Implementation of a Tiered “Scope of Practice”
Instead of a “one-size-fits-all” title, the profession is moving toward clearly defined tiers that restrict certain activities based on qualification levels.
The Solution: Formally designating diploma holders as “Foundational” or “Associate” practitioners. Under this model, diploma holders are restricted from treating high-risk clinical cases (such as active suicidality or severe eating disorders) and must instead focus on early intervention, wellness coaching, and grief support.
The Impact: This protects the public by ensuring high-complexity cases are handled by degree-qualified clinicians while allowing diploma holders to thrive in lower-intensity roles.
B. Mandatory “Step-Up” Supervision and Mentorship
To bridge the gap in theoretical knowledge, diploma holders can be subjected to more rigorous clinical oversight.
The Solution: Increasing the required supervision ratio for Level 1 (Diploma) members. While a Masters-level counsellor might require one hour of supervision per 20 client hours, a diploma holder could be required to have one hour per 10 client hours for the first two years of practice.
The Impact: Regular, high-frequency oversight by a more experienced clinician acts as a “safety net,” catching potential misdiagnoses and providing on-the-job theoretical training.
C. Articulation Pathways (The “Bridge” to Degree)
The “cons” of a diploma are often temporary if the practitioner is encouraged to keep learning.
The Solution: Creating seamless “Articulated Pathways” between TAFEs and Universities. For example, a Diploma of Counselling should provide a full year of credit toward a Bachelor of Counselling.
The Impact: This transforms the diploma from a “dead-end” qualification into an entry-level apprenticeship. It allows practitioners to start working and gaining experience while they study for the higher credentials required for professional status and Medicare eligibility.
D. Targeted National Standards and Regulation
The 2025/2026 push for National Standards for Counsellors and Psychotherapists seeks to unify the industry under one banner while recognizing different “Career Stages.”
The Solution: The standards create a “Stage 1” descriptor for AQF 5-6 qualifications. This includes mandatory “Ethics and Quality Assurance” modules that specifically address the gaps in research literacy and clinical safety found in standard vocational training.
The Impact: By standardising the “add-on” requirements for diploma holders, the ACA can improve the baseline credibility of the entire register, making a stronger case for government recognition.
Summary Comparison: The AQF Divide
Factor
Diploma (AQF 5)
Degree (AQF 7/9)
Primary Philosophy
Vocational competency & speed
Clinical depth & academic rigour
Entry Barrier
Low (TAFE/Private RTO)
High (University/ATAR)
Workforce Impact
Rapid scaling & frontline support
Specialized clinical intervention
Medicare Potential
Almost zero in the current climate
The primary focus of professional lobbying
Career Longevity
Limited; may require further study
High; recognized across all sectors
Proposed Tiering
Foundational / Associate
Professional / Clinical
Conclusion: A Profession at a Crossroads
The inclusion of diploma-qualified counsellors represents a fundamental trade-off between accessibility and authority. By implementing solutions like tiered scope of practice, mandatory high-intensity supervision, and articulated degree pathways, the profession can mitigate the risks of “dilution” while retaining the vital benefits of a diverse and responsive workforce. For Australia, the future likely lies in a “collaborative care” model where diploma holders and degree-qualified clinicians work side-by-side, each within a strictly governed and well-defined role.
In the Australian mental health landscape, the distinction between counselling, social work, and psychology is defined not just by education and regulation, but by deeply held philosophical differences. While all three professions aim to improve human wellbeing, they operate from different conceptual frameworks.
1. Core Philosophies and Values
The primary distinction often cited by Australian professional bodies like the Australian Counselling Association (ACA) and the Psychotherapy and Counselling Federation of Australia (PACFA) is the “Inside-Out” vs. “Outside-In” approach.
Profession
Core Philosophy
Primary Lens
Value Stance
Counselling
Inside-Out
The therapeutic relationship and the client’s internal experience.
Humanistic, non-pathologising, and person-centered.
Social Work
Outside-In
The “Person- in- Environment” (systemic) context.
Social justice, advocacy, and human rights.
Psychology
Scientific- Practitioner
Cognition, behavior, and neurological processes.
Evidence-based, diagnostic, and empirically driven.
The Counsellor’s Distinction
Counsellors in Australia often distinguish themselves by their non-pathologising stance. While a psychologist may look for a diagnosis (e.g., Clinical Depression) and a social worker may look for systemic failures (e.g., housing instability), a counsellor focuses on the subjective meaning the client assigns to their life. They value the “here and now” and the power of the therapeutic alliance over clinical intervention.
2. Key Differences
A. Regulation and Title Protection
Psychology: A protected title. In Australia, you must be registered with the Psychology Board of Australia (PsyBA) via AHPRA. It follows a rigid 4+2, 5+1, or Master’s pathway.
Social Work: A self-regulated profession, though “Accredited Mental Health Social Worker” (AMHSW) is a status granted by the AASW that allows for Medicare rebates.
Counselling: Self-regulated via the ACA or PACFA. Unlike “Psychologist,” the title “Counsellor” is not legally protected in Australia, though industry standards require tertiary qualifications (Diploma, Bachelor, or Master’s) for professional registration.
B. Assessment vs. Exploration
Psychologists are trained extensively in psychometric testing and diagnostic assessments (using the DSM-5-TR). Their goal is often to identify a condition and apply a targeted, evidence-based treatment (like CBT).
Counsellors typically eschew formal diagnosis in favour of “case formulation.” They view the client’s distress as a natural response to life events rather than a “disorder” to be cured.
C. Systemic Advocacy vs. Personal Growth
Social Workers are unique in their mandate to intervene in the client’s environment. They may liaise with courts, schools, or housing providers.
Counsellors generally maintain a “sanctuary” space where the focus is exclusively on the individual’s internal growth and emotional processing, rather than external case management.
3. Key Similarities
Despite philosophical differences, the practical application of these roles overlaps significantly in clinical settings:
Evidence-Based Practice: All three professions use recognised modalities such as Cognitive Behavioral Therapy (CBT), Acceptance and Commitment Therapy (ACT), and Mindfulness.
Ethics: All adhere to strict codes of ethics regarding confidentiality, informed consent, and professional boundaries.
Goal of Wellbeing: The ultimate aim for all three is the reduction of psychological distress and the promotion of client autonomy.
Supervision: Practitioners in all three fields are required to undergo regular supervision to maintain their registration and professional standards. Counselling requires clinical supervision within a contract. Psychology requires at least 10 hours of peer consultation. Social recommends all social workers to participate in professional supervision.
4. Summary Table
Feature
Psychologist
Social Worker (AMHSW)
Counsellor / Psychotherapist
Medicare Rebates
Yes (High)
Yes (Moderate)
No (Currently limited/ trialing)
Pathologising?
Yes (Diagnostic focus)
Contextual (Social focus)
No (Humanistic focus)
Primary Tool
Assessments/ Tests
Advocacy/ Case Management
The Therapeutic Relationship
Focus
Dysfunction/ Behavior
Systems/ Environment
Self-Awareness/ Growth
Conclusion
Counsellors in Australia view themselves as the “guardians of the therapeutic relationship.” While they share many tools with their colleagues in psychology and social work, their distinct value lies in seeing the client as a whole person in a state of “becoming,” rather than a patient with a pathology or a service-user with a systemic deficit.
In PACFA/ACA registration renewal time, I sometimes hear registered counsellors and supervisors ask me whether they should renew professional membership, especially with the associated financial costs, the paperwork, and other membership requirements? (I also ask this question at times). However, for private practitioners, the membership renewal cost may be equivalent to three to five hours of paid practice – or less than one full day private practice income. For this price, you agree to submit to professional accountability to maintain supervision, submit to a code of ethics and professional development, contribute financially to the profession and its public standing, future-proof your place in the profession, and maintain your own professional credibility. Are these benefits worth the price of a day’s income? I think so!
(Pictures are from screenshots from the draft training standards)
If you are a member of the Psychotherapy and Counselling Federation of Australia, or the Australian Counselling Association, you will probably have heard about the development of the national standards for counsellors and psychotherapists. These are a result of the Department of Health and Aged Care funding of $300k for Allen + Clarke consulting, to develop minimum standards for the counselling profession.
The draft version was developed from extensive written submissions and interviews, with stakeholders including counsellors and psychotherapists, the two peak bodies, consumers, and other interested stakeholders.
At this time, the draft version is ready for public consultation. It will close on Friday 13 December 2024.
My analysis
In my view, the document is pretty sound. Given the extensive consultation that formed the background for the draft standards, informed mostly by counsellors and psychotherapists and various working groups in the profession, it is unsurprising that the document is not too different to standards and practices in both the Australian Counselling Association (ACA) and in the Psychotherapy and Counselling Federation of Australia (PACFA).
This said, as it is a draft, I wish to offer my recommendations, many of which are informed by colleagues who I have discussed the draft with.
Expectations without protections
The draft rightly highlights minimum expectations for counsellors and psychotherapists, to ensure that the public is both protected from harm and that the profession aligns with government regulatory practices. The background for the standards recognises the important role counsellors and psychotherapists have in supporting Australian mental health and wellbeing. It also attempts to address the inconsistency between the ACA and PACFA in terms of training standards, guidelines, and practice. The aims are to be supported. However, my first concern is that these standards may create an unequal playing field between those who are part of the profession and thus accountable to these standards, and those who practice as counsellors outside of the profession. Skipping to the final focus area 4.1.4 Removal from practice, it highlights that breaches of the standards may lead to a withdrawal of membership. This implies that these standards only apply to registered counsellors (and psychotherapists, but from now on, I’ll just say counsellors as inclusive of both groups), not unregistered counsellors. In other words, registered counsellors who play by the rules can be removed from practice, and unregistered counsellors do not have a mechanism in these standards to be censured for problematic practice.
In addition to the penalisation of only registered counsellors, it may also disincentivise untrained or even trained but unregistered counsellors from joining as members. Why train, why pay membership, why be compelled to pay for monthly supervision, why pay for annual CPD, and why risk your practice by being a member when you can be a counsellor for no cost or risk? It seems the people who play by the rules bear the costs, the expectations and the risks, while those who practice outside of associations don’t have the same risks or costs. And the public is none the wiser as to who are registered or not.
The standards need either apply to all people who identify as counsellors, members or not, or there needs to be special protected titles for those who are registered, such as Registered Counsellors, or Licenced Counsellors. This way, the public may be better able to discern who is registered with the profession of counselling compared with who is not.
Lower trained counsellors treated as equivalent to more thoroughly trained counsellors
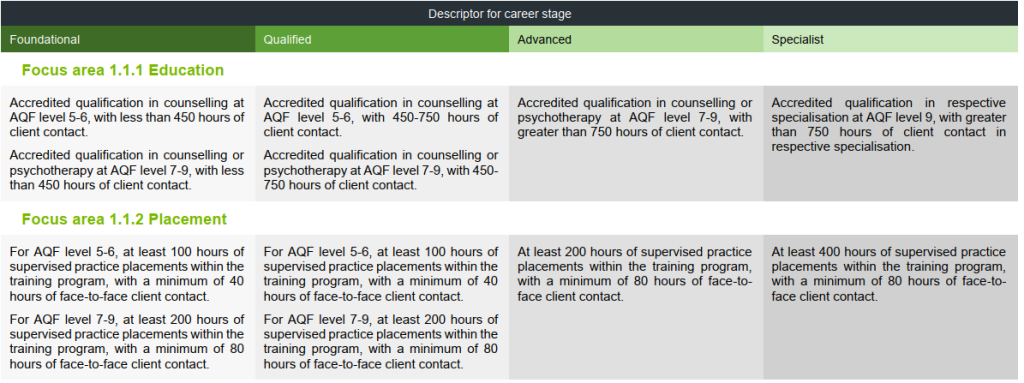
The first focus area that needs reconsideration is on education. The screen shows four columns, each moving from lower levels to higher levels.
The foundational and qualified levels capture diploma, bachelor and Masters level trained counsellors. I see two key issues with listing diploma and degree levels, essentially, as equivalent career stages. Firstly, diploma qualifications, which can be completed in just 12 months, are considered equivalent to degree qualifications that require two to four years of study in terms of level of the lower levels of standing. Secondly, diploma graduates are required to complete fewer placement hours (100) than degree graduates (200 hours). Are lesser qualified, lower trained, and less experienced diploma students really on the same level as degree plus students with more experience? Are the graduates trained as paraprofessionals on the same professional level as those who have had professional training and experience?
To address these concerns, introducing a pre-foundational stage and labeling diploma graduates as “Associate Registered Counsellors” could provide a solution. This distinction would recognise the value of paraprofessionals in counselling, supported by research showing they can achieve equivalent results to professionals. By differentiating associate counsellors from registered counsellors, similar to the nursing profession’s enrolled compared with registered nurses, the counselling profession can enhance credibility and transparency.
This proposed change would have several benefits. It would provide diploma graduates with additional credibility over unregistered counsellors, while clearly communicating their qualifications to the public. It would also address concerns about the reputation of the counselling profession appearing underqualified compared to similar professions that require a minimum of four years of university study. Furthermore, recognising the role of associate counsellors would support Australia’s counselling workforce needs, rather than potentially excluding effective practitioners.
Did COVID never happen?
The draft standards have retained the obsession some have with misconceptions about the importance of face-to-face experience in the formation of counsellors. Placements do not mandate the type of issues, type of therapies, or whether they practice individual, couples, family, or group therapy formats. However, this set of draft standards targets and mandates face-to-face contact, even though the post COVID world has clearly now made other formats of practice delivered via technology, as recognised practice. Existing research on telehealth doesn’t support a face-to-face only-ist position for counsellors. While it finds that face-to-face differs from online and phone therapies, it generally finds equivalent outcomes, therapeutic relationship, and satisfaction for clients. It is not a second-rate practice, though the research indicates that therapists with less experience and knowledge about it, tend to hold incorrect assumptions and negative prejudices against it. Requiring face-to-face only for 80 hours disadvantages students who cannot travel to an agency to do face-to-face work (i.e. remote region students), or who may not intend to become face-to-face practitioners. I wrote an article where I explored relevant research and argued that this restriction is outdated and based on myths. See here. If they maintain the current position, can at least we treat teleconferenced sessions as face-to-face? While not all the body language can be seen, there’s still a lot of body language the counselling practicum student can hear and observe in the interactions. In fact, the proximity of this format of the faces to one another is more literally face-to-face than sitting in a room together a couple of metres apart.
Worried academics – be careful what you wish for?
Another area that might raise eyebrows is the recency of practice. I think this is better labelled Currency of Practice as one could have met the requirements three years ago and not done any practice for the last two years, but still be considered having practiced recently according to this focus area criteria.
From a counselling academic perspective, keeping practice currency can be tricky. While some training institutions make space in the workload, others do not. This can put pressure on academics who are often time poor, working nights and weekends to keep up with their academic workloads, let alone adding practice on top of this.
As an academic, I am not advocating this be dropped even while I know that some of my academic colleagues might oppose this. The first reason is that I believe it is important for academics to maintain currency of practice. I know myself, how fast I become clinically rusty when away from practice for a month or two. I have been practicing for over 25 years and yet I can sense the impact of lengthy breaks. Another reason for keeping it as is, is that having this expectation as a minimum becomes grounds for peak body training standards to require institutions give counsellor educators release for practice, which in turn, should make allowance for in their workloads. Institutions that wish to retain accreditation will need to comply. Giving academics opportunities to maintain practice currency will enable them to provide higher quality current practice experience to speak from, rather than historical experience alone. Should currency of practice be removed, it will disincentivise academics from maintaining it. Being stale and out of touch with practice will in my view, reduce the richness of student experience and lead to academics being out of touch with the realities of contemporary client work. Students often have told me how differently enriching their experience is when taught by practitioners compared to academics without currency of practice. As a practice-based profession, I think we really we need to practice what we teach.
With the CPD criteria proposed, I don’t want to specialise
A colleague recently brought to my attention an issue with the Continuing Professional Development (CPD) requirements. Specifically, specialists who have completed Master’s level training in their area of specialisation are expected to dedicate 20 hours of CPD to that same area, year in, year out. For instance, a specialist drug and alcohol counsellor might be required to focus their professional development exclusively on drug and alcohol-related topics.
This raises concerns for me, as it seems overly restrictive. Clients with specialised concerns, such as addictions, often present with interconnected issues spanning multiple areas, like trauma. By limiting PD options to a single specialisation, practitioners may miss out on valuable training opportunities. While critics of my position might say that I could always do additional CPD in other areas relevant for practice, I would reply that I don’t want to be penalised with a burden of having to do over and above anytime I want to learn something outside of my specialty area. Sorry, this seems like a penalty for being recognised as a specialist. And additionally, it assumes there will always be opportunities for CPD in specialist areas every year. This may not be the case.
Personally, I’m inclined to maintain my advanced status rather than pursue specialist registration, solely to preserve flexibility in my professional development choices.
I recommend revising the CPD requirement to mandate only fewer hours in the specialization area. This adjustment would prevent discouraging professionals from becoming registered specialists, avoiding unnecessary limitations on their PD options, or increased demands.
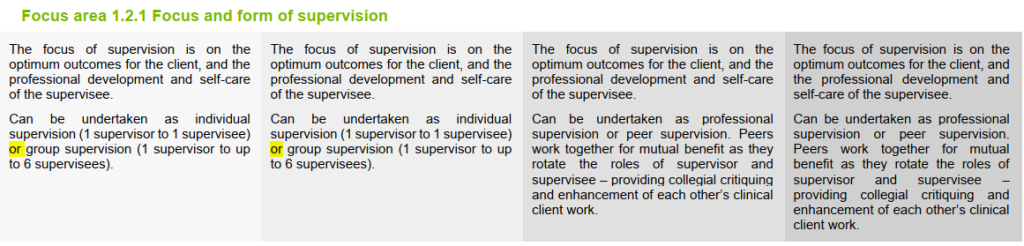
Avoidance or neglect for new counsellors – take your pick
In the standards, less experienced counsellors, including new graduates, don’t have to do individual supervision – at all. While this might save them money, as group supervision is often cheaper, I think this is a risk to the public. An inexperienced counsellor who may not have an opportunity in the group to talk about a difficult client issue that they need help for in the following session is problematic. Moreover, they may be less inclined to bring up more sensitive or embarrassing issues with a group compared to an individual supervisor who is there only for them in the supervision hour, with no witnesses. I have supervised many newly minted counsellors and I know how much individual support they need. I am horrified at this proposal and think it is highly risky.
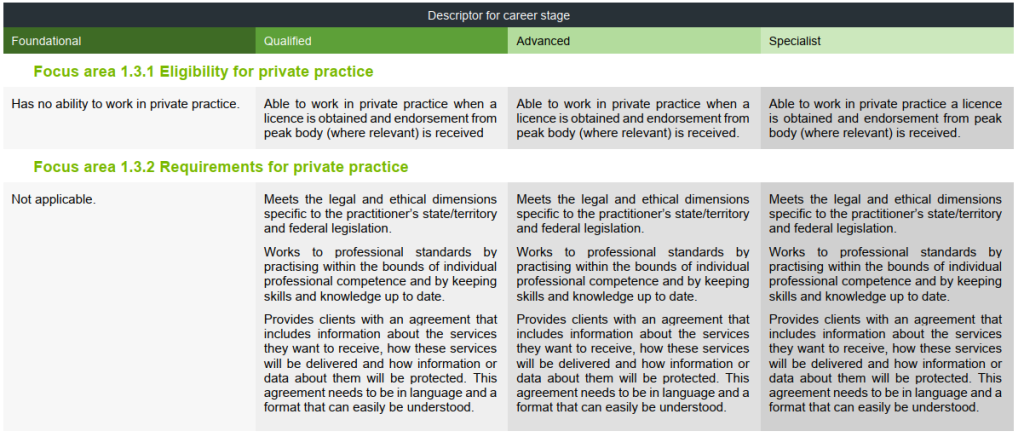
Cheers for supervisor eligibility and private practice restrictions
and
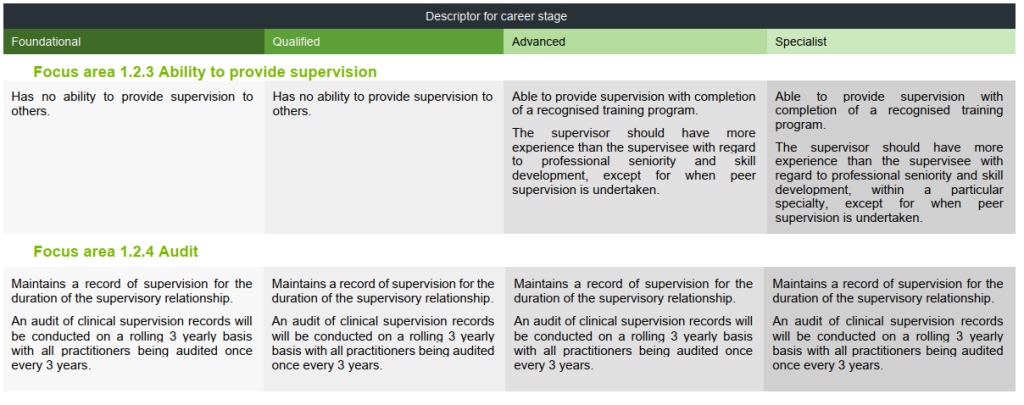
One pleasing update was that foundational and qualified counsellors are unable to provide supervision. This is welcomed to prevent the inexperienced guiding the inexperienced.
There’s also a useful update about eligibility for private practice, wherein there is a recognition that private practice has complexities and risks some with lower qualifications may be less likely to recognise or manage. While there will be some lower qualified and experienced private practitioners who do a great job, these standards address a risk that still continues to this day.
One of the challenges and reasons many counsellors have been attracted to private practice is because the employment market has discriminated against counsellors, making counsellors needing to explore alternative opportunities to practice. I really hope the national standards help to enhance employer respect and willingness to hire counsellors. I appreciate the ACA and PACFA’s efforts to educate industry about what counsellors can do, and both to create Scope of Practice documents as part of this education.
Researching confusion
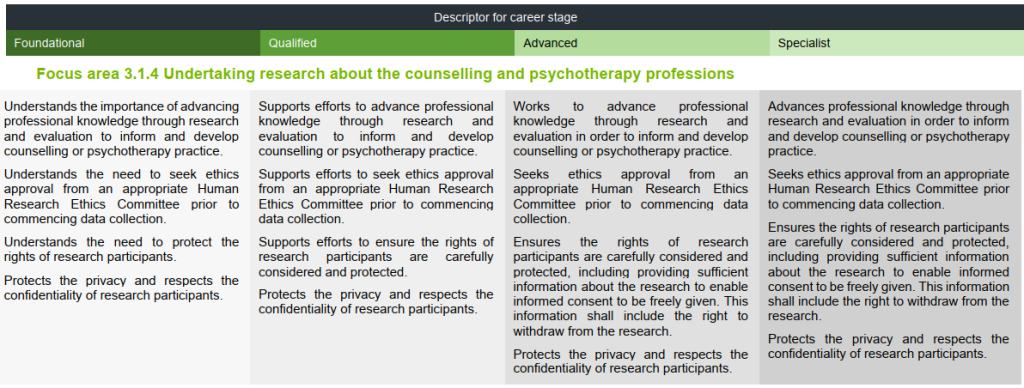
The focus area on research I found somewhat problematic. First, why is the label about undertaking research about the counselling and psychotherapy professions. Why do we need research on the profession as a minimum standard?? Can’t counsellors research other areas related to counselling too?
Also, the section appears to focus on the conducting of research. Firstly, diploma and bachelor students may have between nil and very little research training on average.
The second point I want to make is that rather than focusing on conducting research, shouldn’t require counsellors to be research literate? Very few practitioners will actually conduct and produce research, but all should be able to consume and understand research that might inform their practice. I agree with the importance of what is proposed. I just wonder about its relevance for the lower levels of trained counsellors who are unlikely to have had the relevant training to begin with, and unlikely to gain ethics approval if not having had sufficient research training.
Expert over or collaborate with
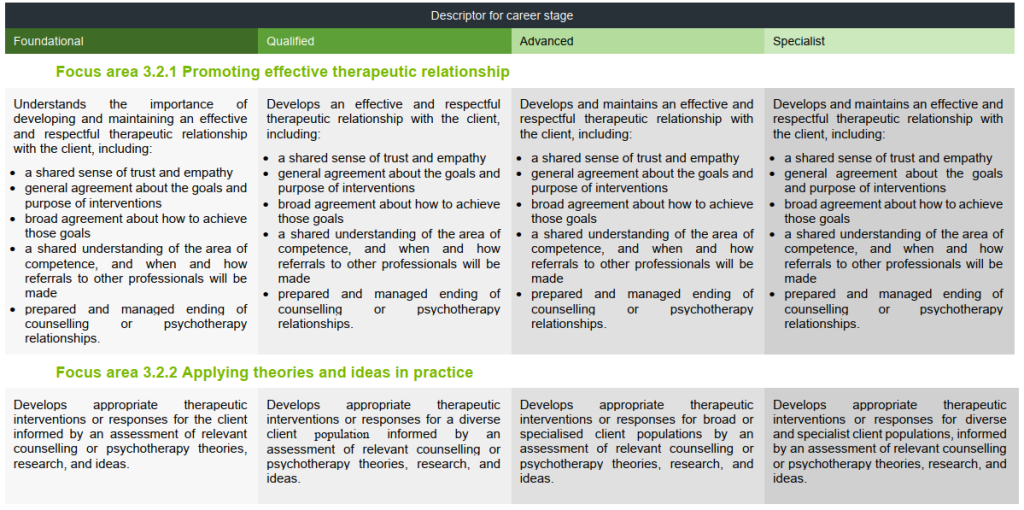
This is my last two areas for critique. 3.2.1 addresses promoting effective therapeutic relationship. First, we don’t promote the effective relationship, as stated in the focus area title. We don’t’ tell clients, “hey, I think you should really enter into a therapy relationship. It’s a really good thing”. No. Counsellors develop or facilitate it. Overall, though, I think this is an important focus area given the counselling profession, in my view, prizes the relationship.
The focus area 3.2.2 on applying theories and ideas in practice. It’s basically saying we should be theoretically informed. No disagreement here. However, the way it is written seems to exclude the client’s voice. In counselling, we do not impose theories or our ideas based on theories onto clients, but there is an interaction between client and counsellor knowledge. It isn’t a top-down expert over process about an interactional process of decision making.
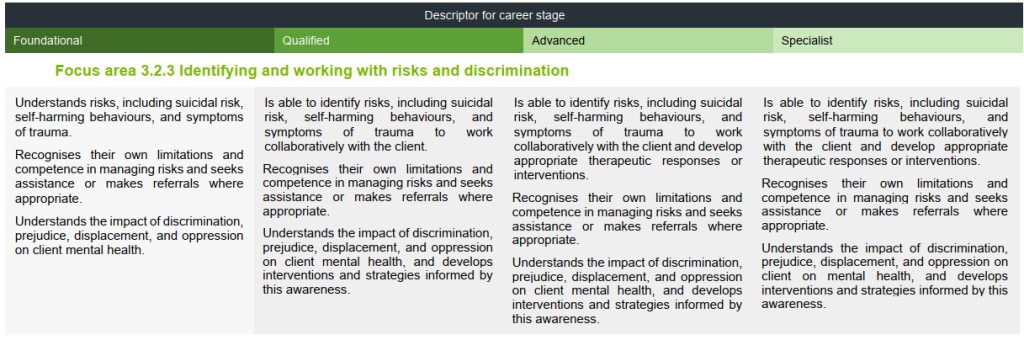
Categorical confusion?
I’m not sure I understand how identifying and working with risks is directly and intrinsically related to discrimination. Focus area 2.1.3 is on respecting diversity, so I would have thought this area is of relevance to the discrimination category. However, I’m happy to be corrected. I just don’t see it at this time.
Conclusion
I’ve listed some of my concerns, not to diminish the perception of the quality of the standards overall, but to highlight some areas that might be worthwhile to reconsider. If you agree with some or all of my points, please use them in your feedback in the survey and share the link to this page with your fellow counsellors.
The counselling profession prizes clinical experience. For counsellors to advance from intern through to clinical member, there is an expectation that they will accrue hundreds of hours of counselling practice over years. Exposure over time to a broader range of clients and their issues, training, professional development, and clinical supervision, is likely to lead counsellors to acquire expanded learning at multiple levels. But does this accruing of experience, knowledge, and skill translate into improved outcomes over time? Or, put another way, will the senior members in the profession be getting better results than they did when they first began their counselling practice?
Goldberg and colleagues (2016) set out to measure therapist performance over time in a longitudinal study. They reviewed the outcome data from 170 therapists from a university counselling service over a period between .44 to 17.93 years (av 4.73). Therapists covered a continuum of career status, from trainee students through to experienced licensed professionals.
The results of the study were surprising. Therapists, as a group, did not improve with experience, whether the experience be measured in time or cases. In fact, overall, there was a very slight decline of outcomes with experience. Breaking it down further, 60% of therapists declined slightly while the remaining 40% improved slightly over time. The bulk of therapists experienced very little improvement or deterioration in their outcomes over time.
How might we interpret these results?
General effectiveness: first, we need to remember that counselling is generally very effective (Smith & Glass, 1977). Finding that counsellor performance generally does not change over time does not suggest clients are not benefitting from treatment. Most clients will benefit from most counsellors.
Staple profession requirements: The results raise questions about the impact on outcomes of professional development and clinical supervision. Both of these areas have little research support on their contribution to improving outcomes. If counsellors are receiving regular supervision and professional development but are not improving in outcomes, we need to understand why. Do these activities simply help us maintain our existing levels of effectiveness? Are benefits of clinical supervision not generalizable across our clients? Or are these activities primarily for other benefits, such as increasing therapist practice knowledge, self-awareness, and resilience?
Over-estimates: Over time, counsellors collectively may not improve in their effectiveness, but they tend to increase in confidence and professional self-belief. Research has demonstrated that therapists over-estimate their effectiveness and typically suffer from self-assessment bias (Walfish, McAlister, O’Donnell, & Lambert, 2012). However, there is some evidence that counsellors who display more professional self-doubt tend to get better outcomes than those who have more professional self-confidence (Nissen-Lie et al., 2017). The interpretation of why this might be the case is that those who lack professional confidence are likely to spend more time devoted to considering their work in comparison to those who engage in less critical professional reflection.
So how can counsellors continue improving their effectiveness? This area of psychotherapy expertise research is still very young. Current suggestions include ensuring appropriate reliable formal outcome feedback is collected. Therapists are typically over-optimistic in their perceptions of client improvement and fail to recognise failing cases (Hannan et al., 2005), hence objective measurement is important. The second is utilising the feedback and translating it into deliberate practice (Goodyear, Wampold, Tracey, & Lichtenberg, 2017), and then checking to see if this deliberate practice converts into improved outcomes.
Counsellors cannot rely on experience, supervision, professional development as pathways to improve their client effectiveness. Current recommendations suggest counsellors need systematic outcome feedback combined with deliberate practice if they seek to continue to improve.
Goldberg, S. B., Rousmaniere, T., Miller, S. D., Whipple, J., Nielsen, S. L., Hoyt, W. T., & Wampold, B. E. (2016). Do psychotherapists improve with time and experience? A longitudinal analysis of outcomes in a clinical setting. Journal of Counseling Psychology, 63(1), 1-11.
Goodyear, R. K., Wampold, B. E., Tracey, T. J. G., & Lichtenberg, J. W. (2017). Psychotherapy expertise should mean superior outcomes and demonstrable improvement over time. The Counseling Psychologist, 45(1), 54-65. doi:10.1177/0011000016652691
Hannan, C., Lambert, M. J., Harmon, C., Nielsen, S. L., Smart, D. W., Shimokawa, K., & Sutton, S. W. (2005). A lab test and algorithms for identifying clients at risk for treatment failure. Journal of Clinical Psychology, 61(2), 155-163.
Nissen-Lie,
H. A., Rønnestad, M. H., Høglend, P. A., Havik, O. E., Solbakken, O.
A., Stiles, T. C., & Monsen, J. T. (2017). Love yourself as a
person, doubt yourself as a therapist? Clinical Psychology & Psychotherapy, 24(1), 48-60. doi:10.1002/cpp.1977
Smith, M. L., & Glass, G. V. (1977). Meta-analysis of psychotherapy outcome studies. American Psychologist, 32(9), 752-760. doi:10.1037/0003-066x.32.9.752
Walfish, S., McAlister, B., O’Donnell, P., & Lambert, M. J. (2012). An investigation of self-assessment bias in mental health providers. Psychological Reports, 110(2), 639-644. doi:10.2466/02.07.17.PR0.110.2.639-644